What you’ll learn in this article…
- Roughly 40 million U.S. adults and 8 percent of children ages 3 to 17 live with a communication disorder.
- Five major types exist: speech sound, fluency, voice, language, and social communication disorders.
- Only about 60 percent of children with speech or language disorders currently receive intervention services.
- Careers in the field range from speech-language pathology assistants to doctoral-level audiologists and researchers.
The boundary between a speech difference and a disorder has never been sharper, or more contested, thanks to updated diagnostic frameworks that now recognize social communication as its own clinical category. Across the United States, roughly 1 in 12 children and millions of adults live with conditions that impair speech, language, or hearing, from childhood apraxia to post-stroke aphasia.
Some communication disorders are present at birth, while others emerge after illness or injury, making a lifespan perspective essential for both diagnosis and intervention. With job openings for speech-language pathologists projected to expand 19% through 2034, understanding these conditions is not just a clinical matter; it's a practical necessity for families, educators, and career changers alike.
What Is a Communication Disorder?
A communication disorder is an impairment in the ability to receive, send, process, or comprehend concepts or verbal, nonverbal, or graphic symbol systems. This definition, established by the American Speech-Language-Hearing Association (ASHA), serves as the foundation for clinical practice and educational policy across the United States. Unlike temporary communication challenges or variations rooted in cultural or linguistic differences, communication disorders represent persistent difficulties that significantly impact daily interaction, learning, and social participation.
Communication Disorders vs. Communication Differences
A critical distinction often overlooked is the difference between a communication disorder and a communication difference. An accent, regional dialect, or use of a language other than English is not a disorder. Similarly, variations in communication style tied to cultural norms, including eye contact patterns, turn-taking conventions, or storytelling traditions, are not pathological. ASHA emphasizes that speech language pathologists must differentiate between disorders requiring treatment and differences that reflect normal linguistic and cultural diversity. Misidentifying a communication difference as a disorder can lead to unnecessary intervention and stigmatization, particularly in multilingual or culturally diverse communities.
The Four Umbrella Categories
Communication disorders encompass four broad categories, each addressing distinct aspects of human communication:
- Speech disorders: Difficulties with articulation, fluency (stuttering), or voice production that affect how sounds and words are formed
- Language disorders: Impairments in understanding (receptive language) or using words, sentences, and social rules (expressive language)
- Hearing disorders: Partial or complete loss of auditory function that disrupts the ability to perceive spoken language
- Social communication disorders: Challenges with pragmatic language use, including reading social cues, taking conversational turns, and adjusting communication style to context
These categories often overlap. A child with a hearing disorder may also develop language delays, while an adult recovering from stroke might experience both speech and language impairments. Conditions like autism spectrum disorder, for example, can affect multiple areas of communication simultaneously; you can learn more about how autism affects communication in our dedicated guide.
Developmental vs. Acquired Disorders
Communication disorders can emerge at any point across the lifespan. Developmental disorders are present from birth or appear during early childhood, often tied to genetic conditions, neurological differences, or unknown causes. Acquired disorders result from injury, stroke, degenerative disease, or trauma later in life. This developmental-acquired distinction shapes treatment planning, prognosis, and the professionals involved in care. A toddler with a phonological delay will follow a different intervention path than a 60-year-old recovering language skills after a cerebrovascular accident, even though both may see a speech-language pathologist. For professionals interested in pursuing this clinical career path, exploring communication disorders master's programs online is a strong first step.
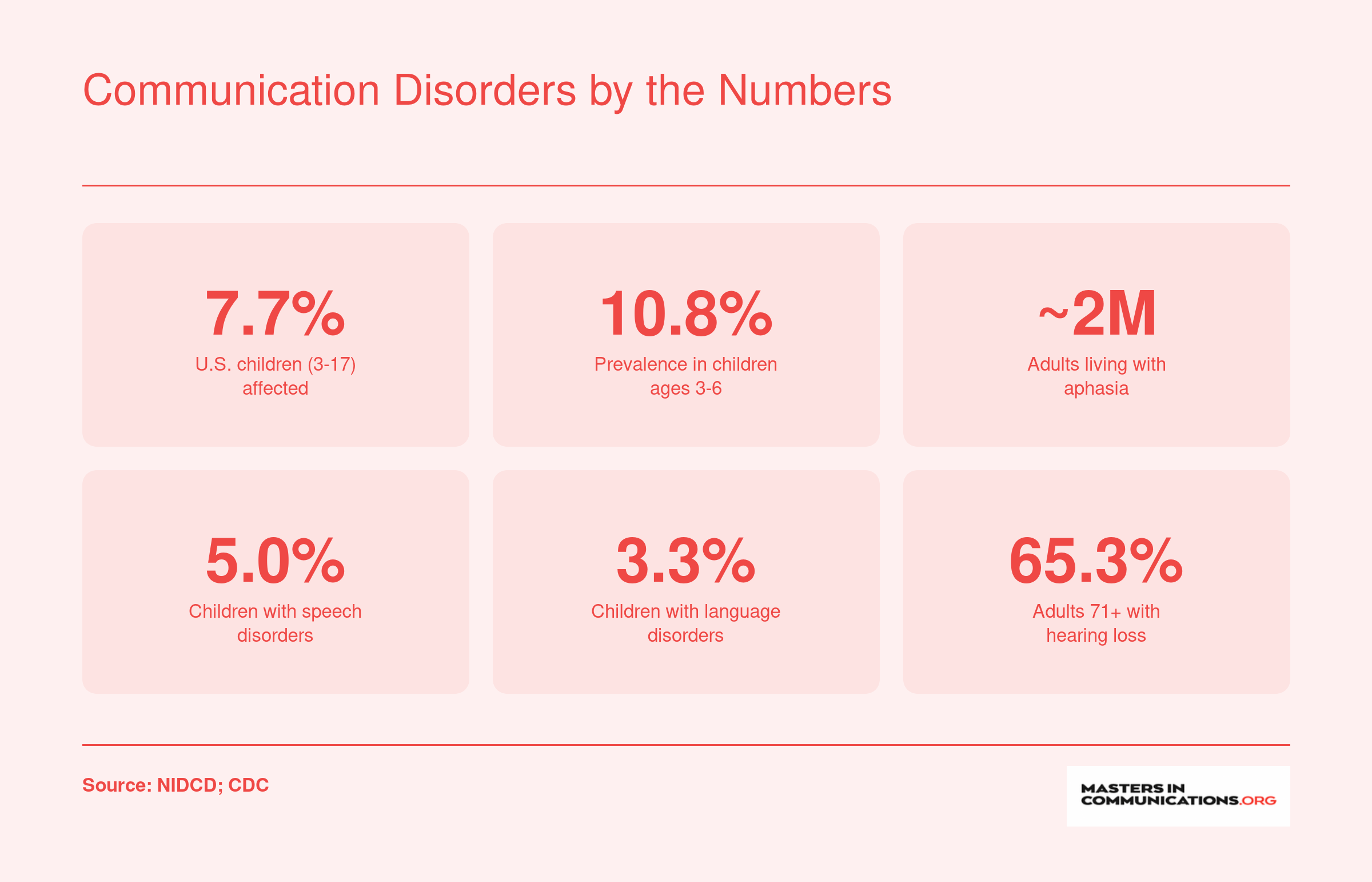
Communication Disorders by the Numbers
Communication disorders affect far more people than most realize, spanning every age group from preschoolers to older adults. These prevalence figures underscore just how widespread these conditions are and why well-trained professionals are in such high demand.
Types of Communication Disorders
Communication disorders span a broad range of conditions that affect how a person produces speech, understands language, processes auditory information, or navigates social interaction. The classifications below draw on frameworks from both the American Speech-Language-Hearing Association (ASHA) and the DSM-5, which overlap considerably but organize certain subtypes differently. This table offers plain-language definitions, common symptoms, and real-world examples so non-clinicians can recognize the major categories.
| Disorder Type | Definition | Common Symptoms | Real-World Example |
|---|---|---|---|
| Articulation Disorder (Speech) | Difficulty producing specific speech sounds correctly, often involving substitutions, omissions, or distortions of consonants or vowels. | Replacing one sound with another (e.g., "wabbit" for "rabbit"), leaving sounds off the ends of words, or producing sounds in a distorted way that is hard to understand. | A seven-year-old consistently says "thun" instead of "sun" and "fee" instead of "three," making classroom participation frustrating for the child and confusing for listeners. |
| Fluency Disorder (Speech) | Disruption in the natural flow, rhythm, or timing of speech. Stuttering is the most well-known fluency disorder; cluttering is another subtype. | Repetitions of sounds or syllables, prolonged sounds, blocks where no sound comes out, visible tension in the face or neck, and avoidance of certain words or speaking situations. | A young professional who stutters may avoid answering the phone at work or substitute words mid-sentence to sidestep a block, which can limit career growth if untreated. |
| Voice Disorder (Speech) | Abnormal pitch, loudness, resonance, or vocal quality that draws attention to itself or makes communication less effective. | Chronic hoarseness, breathiness, a voice that is too loud or too soft, vocal fatigue after brief speaking, and pitch breaks. | A teacher develops vocal nodules from years of projecting in a noisy classroom, resulting in persistent hoarseness that worsens as the school day goes on. |
| Receptive Language Disorder | Difficulty understanding spoken or written language, including vocabulary, sentence structure, and directions. | Trouble following multi-step instructions, difficulty understanding questions, limited vocabulary comprehension, and problems grasping abstract concepts. | A fourth-grader can decode words on the page but struggles to answer comprehension questions because the meaning of complex sentences does not register. |
| Expressive Language Disorder | Difficulty using language to communicate thoughts, needs, or ideas, even when comprehension may be intact. | Limited vocabulary for age, frequent grammatical errors, short or simplified sentences, difficulty retelling a story in order, and word-finding problems. | An adult recovering from a stroke knows exactly what they want to say but produces sentences like "I go store yesterday the milk" because word order and grammar retrieval are impaired. |
| Hearing Disorder | Any degree of hearing loss, from mild to profound, that affects the ability to detect or process spoken language. | Frequently asking others to repeat themselves, turning up the TV volume, difficulty following conversation in noisy settings, delayed speech or language development in children. | A retiree with age-related sensorineural hearing loss gradually withdraws from family dinners because background noise makes it nearly impossible to follow group conversation. |
| Social (Pragmatic) Communication Disorder | Difficulty with the social use of language and nonverbal communication, without the restricted or repetitive behaviors seen in autism spectrum disorder. | Trouble taking turns in conversation, difficulty adjusting language for different audiences, problems understanding sarcasm or implied meaning, and limited use of greetings or eye contact. | A teenager tells a long, detailed story without noticing that the listener has lost interest, and later struggles to understand why a classmate's sarcastic compliment was not sincere. |
| Central Auditory Processing Disorder | Difficulty processing and interpreting auditory information in the brain, even though peripheral hearing is normal. | Trouble distinguishing similar-sounding words, difficulty following spoken directions in noisy environments, frequently mishearing information, and slower response to verbal cues. | A college student passes a standard hearing test but consistently mishears lecture content in a large hall, confusing words like "sixty" and "sixteen" and falling behind on notes. |
Questions to Ask Yourself
Communication Disorders in Children Vs. Adults
Does a child who isn't talking yet have the same kind of communication disorder as an adult who suddenly struggles to find words after a stroke? The short answer is no, and understanding that distinction matters enormously for getting the right help at the right time.
Developmental Disorders: When Communication Doesn't Follow the Expected Path
For children, most communication disorders are developmental in nature. That means the disorder emerges as the child grows, rather than appearing after a period of typical functioning. A three-year-old with a vocabulary of fewer than fifty words, a five-year-old whose speech is largely unintelligible to unfamiliar adults, or a school-age child who avoids conversation due to severe stuttering: these are the presentations clinicians and parents most commonly recognize.
Developmental communication disorders rarely travel alone. Autism spectrum disorder frequently co-occurs with language delays, social communication difficulties, and pragmatic language challenges. Children with hearing loss effects on communication from birth may show delays across speech, language, and literacy if the loss goes undetected. Learning disabilities, intellectual disabilities, and attention disorders can all intersect with communication difficulties, making accurate diagnosis a careful, multi-step process.
Early identification is critical here. The brain's plasticity during the first several years of life means that intervention initiated early tends to produce meaningfully better outcomes than the same intervention started later.
Acquired Disorders: When Communication Changes After Years of Typical Functioning
Adult-onset communication disorders follow a different trajectory, and they receive far less public attention than they deserve. Rather than a skill that never fully developed, an acquired disorder represents a loss of something that once worked. Stroke is among the most common causes, and aphasia is the language disorder most closely associated with it. A person with aphasia may struggle to retrieve words mid-sentence, produce garbled speech despite knowing what they want to say, or have difficulty understanding spoken or written language.
Traumatic brain injury introduces another profile: cognitive-communication deficits that affect attention, memory, and the ability to follow conversations or stay on topic. These deficits can be subtle enough to go unrecognized, yet disruptive enough to interfere with work and relationships.
Neurodegenerative conditions, including Parkinson's disease, ALS, and the dementias, produce their own communication challenges. Dysarthria (reduced motor control of the speech muscles) is common in Parkinson's and ALS, making speech slow, imprecise, or effortful. Dementia progressively erodes word retrieval, comprehension, and the ability to maintain coherent conversation.
The emotional toll of acquired disorders is significant and often underappreciated. Adults who lose communication abilities they once took for granted face a heightened risk of depression and social withdrawal. Isolation compounds the functional impact of the disorder, making psychosocial support a necessary component of comprehensive care alongside speech-language therapy.
Why the Distinction Shapes Treatment
Recognizing whether a disorder is developmental or acquired shapes every aspect of clinical planning: the goals of therapy, the pace of progress expected, the role of family and caregivers, and the measures used to define success. A speech-language pathologist working with a toddler is building skills from the ground up; one working with a stroke survivor is often helping a person reclaim and compensate for what was lost. Both roles are demanding and specialized, which is part of why training in communication disorders spans communication sciences and disorders masters programs that cover clinical education across the lifespan.
Causes and Risk Factors of Communication Disorders
A communication disorder's cause is the specific biological or environmental trigger that disrupts typical speech, language, or hearing development or function. Risk factors are characteristics that increase the odds of developing such a disorder, though they may not act alone. Understanding these layers helps focus prevention and early intervention.
Genetic and Hereditary Factors
Some communication difficulties run in families, pointing to genetic influences. A family history of stuttering, specific language impairment, or congenital hearing loss can significantly raise a person's own risk. Researchers have identified gene mutations linked to inherited deafness and certain speech-sound disorders, though the inheritance patterns are often complex and not yet fully mapped.
Neurological Conditions
Damage or differences in the brain's communication centers can disrupt any piece of the process, from forming words to interpreting meaning. - Stroke: A leading cause of aphasia in adults, where language comprehension or production is impaired after a cerebrovascular accident. - Traumatic brain injury: Can affect cognitive-linguistic skills, motor speech planning, or social communication. - Cerebral palsy: Often involves dysarthria due to weak or uncoordinated speech muscles. - Autism spectrum disorder: Frequently includes social communication challenges and pragmatic language deficits.
Structural Differences
Physical abnormalities in the oral, nasal, or hearing structures can directly interfere with speech and hearing. Cleft palate, even after surgical repair, may alter resonance and articulation. Vocal cord nodules or polyps can cause hoarseness or voice loss. Malformations of the outer or middle ear can result in conductive hearing loss, while cochlear anomalies may produce sensorineural hearing loss.
Environmental and Modifiable Risks
Some risk factors are within our power to change or manage. Chronic middle-ear infections (otitis media) during critical language-learning years can muffle hearing long enough to delay speech and language milestones. Prolonged exposure to loud noise, whether occupational or recreational, damages hair cells in the inner ear and leads to permanent hearing loss. To understand more about the impact of hearing loss on communication, it helps to recognize that even mild, temporary hearing changes can compound over time. A lack of language-rich interaction in early childhood, sometimes tied to limited caregiver responsiveness or low socioeconomic access to stimulating environments, can slow vocabulary growth and sentence development. - Untreated ear infections: Can cause fluctuating hearing loss that disrupts language acquisition. - Noise exposure: Use of hearing protection and volume limits helps prevent noise-induced hearing loss. - Limited verbal engagement: Programs that coach parents in interactive reading and conversation can mitigate this risk.
Multifactorial Origins and High-Risk Groups
For many childhood communication disorders, no single cause can be pinpointed. Instead, a combination of genetic susceptibility, subtle neurological differences, and environmental influences interact, a model often called multifactorial etiology. Certain populations face elevated risk: - Premature infants: Often have underdeveloped auditory systems and may face additional medical complications that affect communication. - Children with autism or genetic syndromes: Frequently experience co-occurring language delays or speech difficulties. - Adults post-stroke: Face a sharply higher likelihood of aphasia, apraxia, or dysarthria depending on lesion location and size.
This interplay across the lifespan underscores why diagnosis and treatment must be highly individualized, considering both inherent biology and the opportunities or exposures a person encounters.
How Communication Disorders Are Diagnosed
Diagnosing a communication disorder is a structured, collaborative process that typically unfolds over two to four weeks, though complex cases may take longer. A speech-language pathologist (SLP) usually leads the evaluation, often working alongside an audiologist and, when social communication concerns arise, a multidisciplinary team that may include a psychologist or developmental pediatrician. Clinicians draw on validated instruments such as the CELF-5 for core language ability in individuals ages 5 to 21, the Goldman-Fristoe Test of Articulation-3 for speech-sound accuracy, the ADOS-2 for social communication patterns, and the PLS-5 for preschool-age language development. Additional tools like the PPVT-5, TOLD, and the Boston Diagnostic Aphasia Examination help round out the picture for vocabulary, spoken language, or acquired language loss in adults.
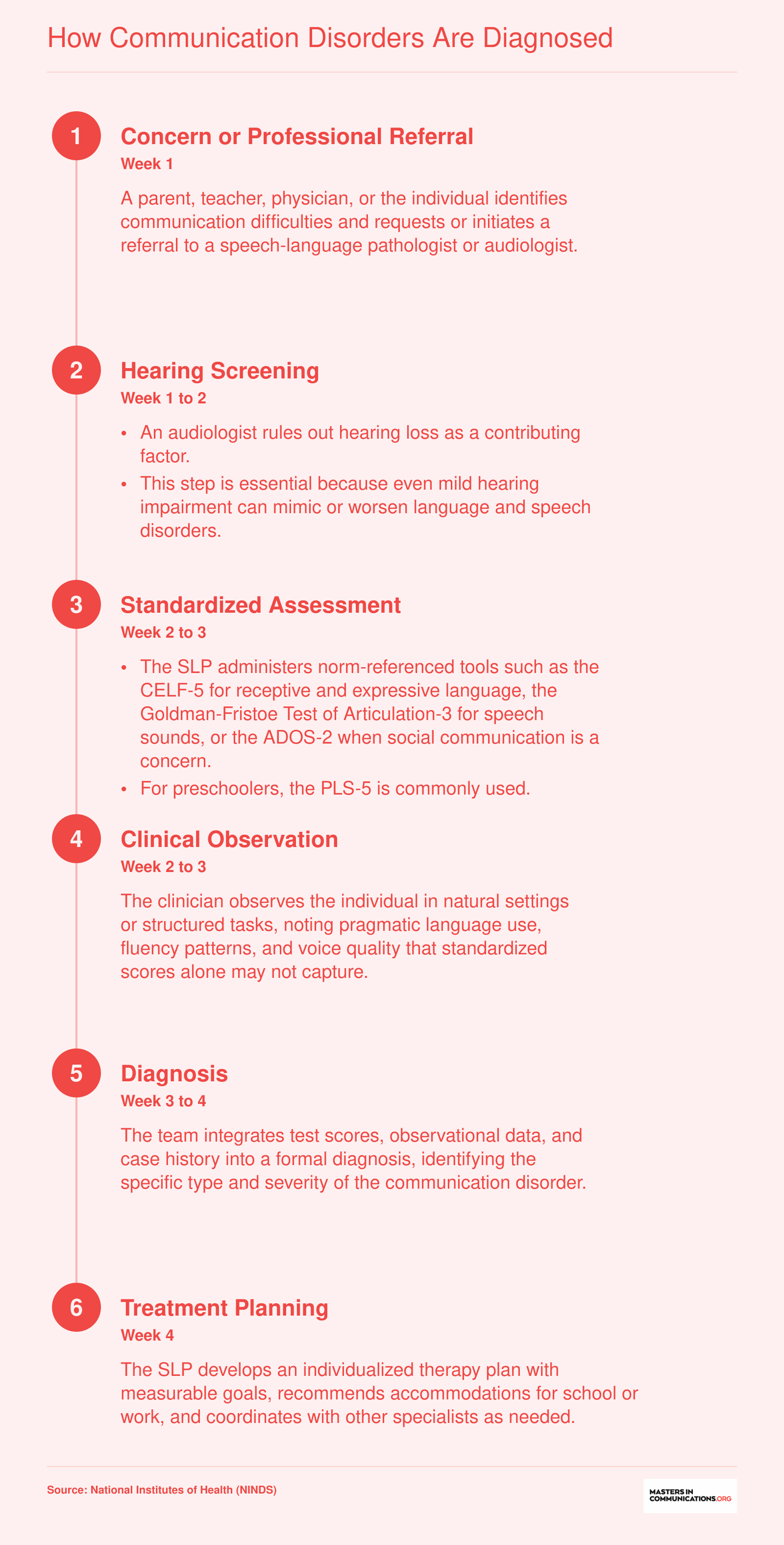
According to data from the National Health Interview Survey analyzed by NIDCD, only about 60 percent of children with voice, speech, or language disorders receive intervention services. For children specifically with voice disorders, the gap is even more striking: just 22.8 percent receive treatment, leaving the vast majority without professional support.
Evidence-Based Treatment and Therapy Options
The treatment landscape for communication disorders has shifted dramatically in the past few years, with telepractice becoming a mainstream delivery model and augmentative technology reaching levels of sophistication that were hard to imagine a decade ago. What has not changed is the core principle: early, evidence-based intervention produces measurable gains, and the research base supporting that claim continues to grow.
Individual Speech-Language Therapy
One-on-one sessions with a speech-language pathologist (SLP) remain the most widely used treatment modality. The clinician tailors targets, cues, and practice intensity to the individual's profile, making it ideal for clients with complex or co-occurring disorders. A 2024 systematic review and meta-analysis examining 23 studies of interventions for children with developmental speech and language disorder found medium-to-high effect sizes for phonological accuracy, confirming that structured, individualized therapy yields clinically meaningful improvement.1 Earlier meta-analytic work established that a minimum of eight weeks of therapy is generally needed before reliable gains emerge in children with primary speech and language delays.2
Group Therapy and Parent-Guided Approaches
Group therapy places clients with similar goals in a shared session, encouraging naturalistic conversational practice and peer modeling. It is especially effective for pragmatic language targets, fluency management, and social communication skills. A 2022 meta-analysis of language therapy for children with developmental language disorder (DLD) reported an overall effect size of 0.46 for expressive language gains, but parent-guided interventions showed a notably stronger effect (1.12) compared with clinician-only models (0.23).3 That finding underscores how involving caregivers in therapy, whether through coaching or structured home practice, can amplify outcomes considerably.
The same meta-analysis found effect sizes of 0.43 for expressive vocabulary, 0.62 for number of different words used, and 2.16 for mean length of utterance, illustrating that therapy can move multiple language dimensions at once when intensity and caregiver involvement are optimized.3
Telepractice and Its Expansion of Access
Telepractice, or teletherapy, exploded in adoption during the early 2020s and has since become a permanent fixture of clinical service delivery. Research consistently shows comparable outcomes between telepractice and in-person sessions for articulation, language, and fluency therapy. For rural communities, underserved urban neighborhoods, and families juggling complicated schedules, teletherapy removes geographic and logistical barriers that once delayed or prevented treatment entirely. Many school districts and early intervention programs now offer hybrid models that blend in-person evaluation with ongoing remote therapy sessions.
Augmentative and Alternative Communication (AAC)
AAC encompasses every tool and strategy that supplements or replaces spoken language for individuals who cannot rely on speech alone. The technology spans a wide spectrum:
- Low-tech options: Picture exchange boards, alphabet boards, and symbol charts require no batteries and work in virtually any setting.
- Mid-tech devices: Single-message or sequential-message buttons give users a voice with minimal cognitive load.
- High-tech solutions: Speech-generating devices and tablet-based apps such as Proloquo2Go, TouchChat, and TD Snap use dynamic displays, word prediction, and synthesized speech to support robust, flexible communication.
AAC benefits a broad population: children with autism spectrum disorder, adults with amyotrophic lateral sclerosis (ALS), stroke survivors with severe aphasia, and anyone whose natural speech is insufficient to meet daily communication needs. Modern AAC systems are increasingly customizable, allowing clinicians to program vocabulary sets that reflect a user's routines, interests, and cultural context.
Adult-Specific Treatment Approaches
Adults face a distinct set of communication challenges, and treatment protocols reflect that reality.
For aphasia following stroke, constraint-induced language therapy (CILT) restricts compensatory gestures and writing to force verbal output, producing gains in naming and spontaneous speech when delivered at high intensity. Script training takes a different angle, helping individuals rehearse personally relevant conversational scripts until delivery becomes automatic and natural sounding.
Cognitive-communication therapy addresses the attention, memory, and executive-function deficits that often accompany traumatic brain injury (TBI). Clinicians use structured tasks, metacognitive strategy training, and real-world simulations to rebuild the cognitive scaffolding that supports effective communication.
Voice therapy targets laryngeal disorders such as vocal nodules, muscle tension dysphonia, and unilateral vocal fold paralysis. Techniques like resonant voice therapy and vocal function exercises retrain the way a person produces sound, often reducing or eliminating the need for surgical intervention.
Across all of these modalities, the evidence points to the same conclusion: intensity matters, individualization matters, and involving the client's support network, whether that means family members, educators, or workplace colleagues, consistently strengthens outcomes.
Living With a Communication Disorder: Accommodations and Support
Living with a communication disorder often means navigating a world where everyday interactions, ordering coffee, participating in a meeting, reading a story to a child, carry hidden hurdles. The right accommodations, strategies, and support networks can transform that experience, opening doors to fuller participation in school, work, and community life.
School-Based Accommodations for Children
For children, federal laws like the Individuals with Disabilities Education Act (IDEA) and Section 504 of the Rehabilitation Act mandate free, appropriate public education and equal access. An Individualized Education Program (IEP) provides specialized instruction and services such as speech-language therapy, while a 504 plan offers accommodations like extended time on tests, preferential seating, or access to assistive technology. Common classroom tools include speech-generating devices, text-to-speech software, and visual schedules that support language processing. Parents should work closely with the school team, including speech language pathology professionals, teachers, and administrators, to ensure the plan matches their child's evolving needs.
Workplace Strategies and Your Rights Under the ADA
The Americans with Disabilities Act (ADA) protects qualified individuals with communication disorders from discrimination and requires reasonable accommodations by employers with 15 or more employees.1 The law recognizes speaking, hearing, reading, communicating, and concentrating as major life activities.1 Reasonable accommodations might include: - Quieter workspace: Reducing background noise to ease concentration and verbal interactions. - Assistive technology: Speech-to-text apps, amplified phones, or communication boards. - Meeting modifications: Providing written agendas in advance, allowing written responses, or using captioning services. - Flexible communication methods: Substituting phone calls with email or instant messaging.
Employees can access free guidance from the Job Accommodation Network (JAN), while the ADA National Network offers training and technical assistance.1 The U.S. Equal Employment Opportunity Commission (EEOC) enforces ADA provisions and can guide you through the process of requesting accommodations.2
Self-Advocacy and Home Practice
Self-advocacy starts with understanding your rights and clearly articulating your needs. For children, parents can model this by practicing conversation scripts, rehearsing how to ask a teacher for extra time, or keeping a communication journal. At home, families can build skills through structured activities: parents of children with speech delays might use picture cards during mealtime to reinforce vocabulary, while adults with aphasia benefit from communication partner training, a technique taught by professionals from organizations like the National Aphasia Association that teaches spouses and friends to slow down, use unspoken communication cues like gestures, and confirm understanding.
Protecting Mental Health and Finding Community
The daily frustration of being misunderstood can contribute to social isolation, anxiety, and depression. Acknowledging this emotional toll is essential, and health communication resources can help families and professionals address these concerns. Support groups provide a non-judgmental space to share experiences and learn coping strategies. The National Stuttering Association connects people who stutter through local chapters and annual conferences, while the National Aphasia Association offers online communities and resource directories. These networks remind individuals and families that they are not alone, turning shared challenges into collective strength.
Career Paths in Communication Disorders
What jobs can you get with a degree in communication disorders, and what does each path require?
The field of communication disorders supports multiple distinct career tracks, ranging from entry-level clinical support roles to doctoral-level independent practice. Understanding the degree requirements and earning potential of each can help you decide where to invest your education.
Speech-Language Pathologist
Speech-language pathologists are the cornerstone of this field. They assess and treat a wide range of speech, language, voice, fluency, and swallowing disorders across the lifespan. Entry into the profession requires a master's degree in communication sciences and disorders, followed by a clinical fellowship and state licensure. Most states also require the Certificate of Clinical Competence (CCC-SLP) from the American Speech-Language-Hearing Association.
According to the Bureau of Labor Statistics, the national median annual wage for SLPs was $95,410 in 2024, with roughly 187,400 professionals employed across the country.1 The field is growing fast: the BLS projects a 15 percent increase in SLP jobs between 2024 and 2034, a rate far above the average for all occupations.1
Audiologist
Audiologists specialize in diagnosing and managing hearing, balance, and related auditory disorders. The entry-level credential is now a clinical doctorate (Au.D.), a four-year graduate program that includes supervised clinical hours. National median annual wages for audiologists reached $95,590 in 2024, nearly identical to SLP earnings.2 Total employment stands at around 14,700, and the BLS projects 11 percent job growth through 2034.2
Speech-Language Pathology Assistant
For those who want to enter the workforce sooner, the speech-language pathology assistant (SLPA) role offers a faster pathway. An associate's degree plus a supervised training program and required clinical experience is the typical preparation.3 SLPAs work under the supervision of licensed SLPs, carrying out treatment plans rather than designing them. Salaries generally fall between $40,000 and $60,000 nationally, depending on setting and experience.3
Collaborative and Adjacent Roles
SLPs rarely work in isolation. Special education teachers, rehabilitation counselors, and occupational therapists all intersect with communication disorders regularly, particularly when serving clients with complex or co-occurring needs. Professionals in these roles benefit from a foundational understanding of communication science even when their primary license sits in a different discipline. You can explore a broader view of careers with a masters in communication to see how these adjacent paths connect.
Exploring Graduate Programs
If any of these paths sounds like the right direction, the logical next step is exploring accredited masters in communication sciences and disorders programs. Accreditation through ASHA's Council on Academic Accreditation (CAA) is a key quality marker to look for, and comparing program options, admissions requirements, and clinical placement opportunities will help you find the best fit for your goals.
Frequently Asked Questions About Communication Disorders
Whether you are exploring this topic for the first time or considering a career helping people with communication difficulties, these answers address the questions professionals and families ask most often.
- What are the 4 types of communication disorders?
- The four primary types are language disorders (difficulty understanding or producing language), speech sound disorders (problems with articulation or phonological patterns), childhood-onset fluency disorder (stuttering), and social (pragmatic) communication disorder (challenges using language appropriately in social contexts). Some classification systems also include voice disorders, but these four categories form the core framework used in clinical diagnosis.
- What is the difference between a communication disorder and a communication difference?
- A communication difference reflects variations shaped by culture, dialect, accent, or multilingualism and does not impair a person's ability to function effectively within their own community. A communication disorder, by contrast, involves a measurable impairment in speech, language, or social communication that limits participation in daily life. Clinicians must distinguish between the two to avoid misdiagnosis, especially in linguistically diverse populations.
- How are communication disorders diagnosed in adults?
- Adult diagnosis typically begins with a referral to a speech-language pathologist, who conducts standardized assessments of speech production, language comprehension, fluency, voice quality, and cognitive communication skills. Medical evaluations, including neurological imaging, may follow when stroke, traumatic brain injury, or degenerative conditions are suspected. Case history interviews and functional communication measures help pinpoint how the disorder affects work, relationships, and daily routines.
- Can communication disorders be cured?
- Some communication disorders, particularly those identified early in childhood, can be resolved entirely through targeted speech-language therapy. Others, such as those caused by neurological injury or progressive conditions like Parkinson's disease, may not be fully curable but can be managed effectively. Evidence-based interventions, augmentative and alternative communication devices, and ongoing support often lead to significant functional improvement even when a complete cure is not possible.
- What causes communication disorders in children?
- Causes range from genetic and neurological factors (such as Down syndrome or autism spectrum disorder) to hearing loss, premature birth, and environmental influences like limited language exposure. In many cases, the exact cause is unknown. Frequent ear infections during critical language-development windows can also contribute. Early identification through developmental screening is essential because timely intervention produces the strongest long-term outcomes.
- What careers work with people who have communication disorders?
- Speech-language pathologists and audiologists are the primary professionals in this field, but the broader workforce includes special education teachers, occupational therapists, clinical psychologists, and rehabilitation counselors. A master's degree is the standard entry point for speech-language pathology, while audiologists typically need a doctoral degree. Career demand remains strong: the Bureau of Labor Statistics projects faster than average job growth for both SLP and audiology roles through the end of the decade.